









-
 Warranty Period
Warranty Period
-
 20+ years in business
20+ years in business
Value of Our Custom Healthcare Development Services
HealthTech clients trust Belitsoft to develop their healthcare software products, from idea implementation to maintenance, and modernization. The goal is to make these products more attractive to medical organizations, drive sustained growth, and expand market reach.
We augment client teams by adding expert healthcare software developers to accelerate project timelines and foster innovation and leadership in healthcare technology.
Let's Talk Business- Be interoperable, analytics-rich, cloud-native, AI & ML-powered, IoT-integrated, up-to-date, and cross-platform compatible
- Handle large data inputs and increased usage without degrading performance
- Strictly secure sensitive patient data
- Comply with HIPAA and other healthcare standards
Custom Healthcare Software Development Services
 Healthcare Software Development Outsourcing
Healthcare Software Development Outsourcing
Outsource custom medtech software development to our medical software developers, who have software engineering skills and understand the healthcare domain. We offer a full range of product engineering services: custom healthcare software development from the ground up, prototyping, and add-on development. Our team of healthcare software developers and dedicated QA resources ensures both software usability and strict compliance with regional and industry standards.
 Healthcare Cloud Development Services
Healthcare Cloud Development Services
Our team experienced in custom healthcare technology software development builds complex cloud-based custom healthcare software products leveraging deep domain expertise in cloud-driven healthcare software engineering, including cloud migration services (migration of existing software systems to the cloud platforms like Microsoft Azure, Amazon Web Services, Google Cloud platform, and others).
We specialize in creating a diverse range of healthcare software tailored to meet the unique needs of your healthcare-related business.

Health Data & Analytics Software Development
AI Clinical Documentation Solutions
For pioneers in generative AI products for healthcare aiming to improve clinical documentation efficiency, we provide data, platform, and infrastructure engineers to build AI-powered platforms for medical conversations that transform patient-clinician interactions into structured clinical notes in real time, with deep EMR integrations (Epic, Athena, AllScripts, Cerner, eClinicalWorks, NextGen, and others). Our medical NLP experts, experienced in conversation summarization, evidence extraction, and outcome prediction, are ready to support the expansion of your fast-moving startup during its hyper-growth phase.
LLMs for Healthcare
For companies developing safety-focused Large Language Models for healthcare, Belitsoft offers software engineers to build and optimize the data infrastructure powering their ML operations, as well as to design and scale reliable, data-driven services for ML model training, data processing, and deployment. Our solution architects ensure successful product implementations, while our site reliability engineers design and implement infrastructure automation, continuous integration and delivery pipelines, and monitor and scale the infrastructure supporting your healthcare AI platform.
Population Health Data Platforms
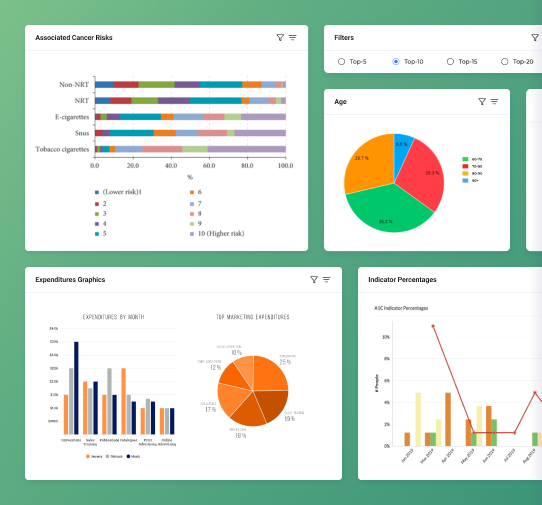
We are ready to build the most amazing products to help you become the most impactful healthcare performance improvement company in clinical, operational, and financial areas by integrating data into a flexible platform and delivering analytic applications based on it. Our highly skilled engineers apply their knowledge of Python, cloud platforms (AWS, Azure, or Google Cloud), data processing tools and techniques (SQL, NoSQL databases, data pipelines, and ETL processes). They work with EHR, claims, imaging, labs, and other real-world data to build descriptive, predictive, and prescriptive analytical models. Along with Business Intelligence consultant for Healthcare, our data analysts, developers specialized in healthcare data visualization (experts in cleaning, analyzing, reporting) help you build the next generation of dashboards, and reports for your customers in the provider/payer market, utilizing cloud (Redshift, Azure, Snowflake, etc.) and traditional OLTP database platforms (Postgres, MS SQL Server, among others). Belitsoft’s experts cover the full project lifecycle from pitch, prototyping, and design to build, integration, QA, and delivery.
Health Information Exchange
Belitsoft’s engineers help leading companies develop interoperability API-first (FHIR) platforms that facilitate secure data transactions of patient encounter details, lab results, billing information between provider-to-provider, provider-to-health-insurance companies, as well as among health systems, payers, and patients. We assist startups and enterprises in developing custom platforms that enable their customers in health IT, value-based care, and digital health to access, integrate, aggregate, and share data by connecting to multiple networks, EHRs, and interoperability frameworks. This includes platforms that support risk adjustment optimization, HEDIS and Star ratings improvement, regulatory compliance, and workflows for enrollment, provider outreach, data retrieval, coding, reporting, submissions, and risk and quality management programs. Our healthcare software developers have experience building and maintaining web applications in commercial settings, including backend systems, RESTful APIs within a microservice architecture, cloud, and healthcare interoperability technologies. They also implement advanced cybersecurity measures.
Real-World Data Software
We help real-world patient clinical data providers create proprietary platforms or suites of web-based tools, combining real-time access to longitudinal clinical data with state-of-the-art analytics. These tools are designed to answer complex research questions at the speed of thought, generate fit-for-purpose cohorts, maximize clinical trial success, and ensure new therapies reach the right patients. Our software engineers tackle scaling challenges that come with building applications transacting with petabytes of molecular data and clinical imagery. They propose cloud-based architectures to address these challenges and implement these designs across a graph of microservices. They also build solutions to process health data, de-identifying it at an unprecedented scale while preserving patient privacy in compliance with legal guidelines. Belitsoft’s engineers possess the required skills in modern frontend technologies, such as React, Angular, and have coding experience with backend languages as Python and Java. They design and implement scalable, highly available, cloud-based applications that handle terabytes or even petabytes of data.
Digital Health Insurance platforms
Our top-notch senior engineering team builds reliable and maintainable custom full-stack technology platforms, core applications, next-generation infrastructure, and interfaces for innovative health insurance companies to make interacting with healthcare systems easier for their members and providers. They also implement stepwise technical migrations of existing services and applications. We optimize data processing pipelines, enhance payment processing, scale claims systems to adjudicate millions of claims per day, and leverage machine learning to identify fraud, waste, and abuse in claims, ensuring high system reliability and performance, improving system integrity, enabling new levels of analytical decision-making, and supporting cost-saving measures.
Healthcare Data Migration
Our data migration engineers specialize in transitioning from legacy systems to new platforms, bringing expertise in data querying, ELT, data modeling, and BI tools. They handle tasks such as migrating and re-engineering data marts in Databricks, optimizing Databricks queries for peak performance, building or updating BI applications to align with the new platform, identifying and resolving issues during migration, and validating results. We transfer client data marts and reports, refactor or develop new components of legacy data models, repoint the BI layer with new measures and visualizations, and help to switch between visualization tools (e.g., Power BI to Tableau, Qlik).
Healthcare Software Modernization
Modernize your EHR or other health information system with Belitsoft through application modernization by adding new features and securing the software for years. Get a better version of your profitable web/mobile product that is highly customizable, flexible and scalable. We'll help your healthtech company migrate the backend and frontend of your flagship products from obsolete frameworks, and achieve certifications. Our developers can convert it to a resilient, secure cloud-native software (AWS/Azure) from a desktop-based and on-premise. To improve performance, we refactor or rewrite the code, optimize the database, and integrate new APIs.
our healthcare developers offer a combination of deep back-end expertise and a tailored approach

Build custom patient recruitment software to recruit enough cases for a trial on time. Speed up and automate the time-consuming process of recruitment, screening, and management of patients for clinical trials.

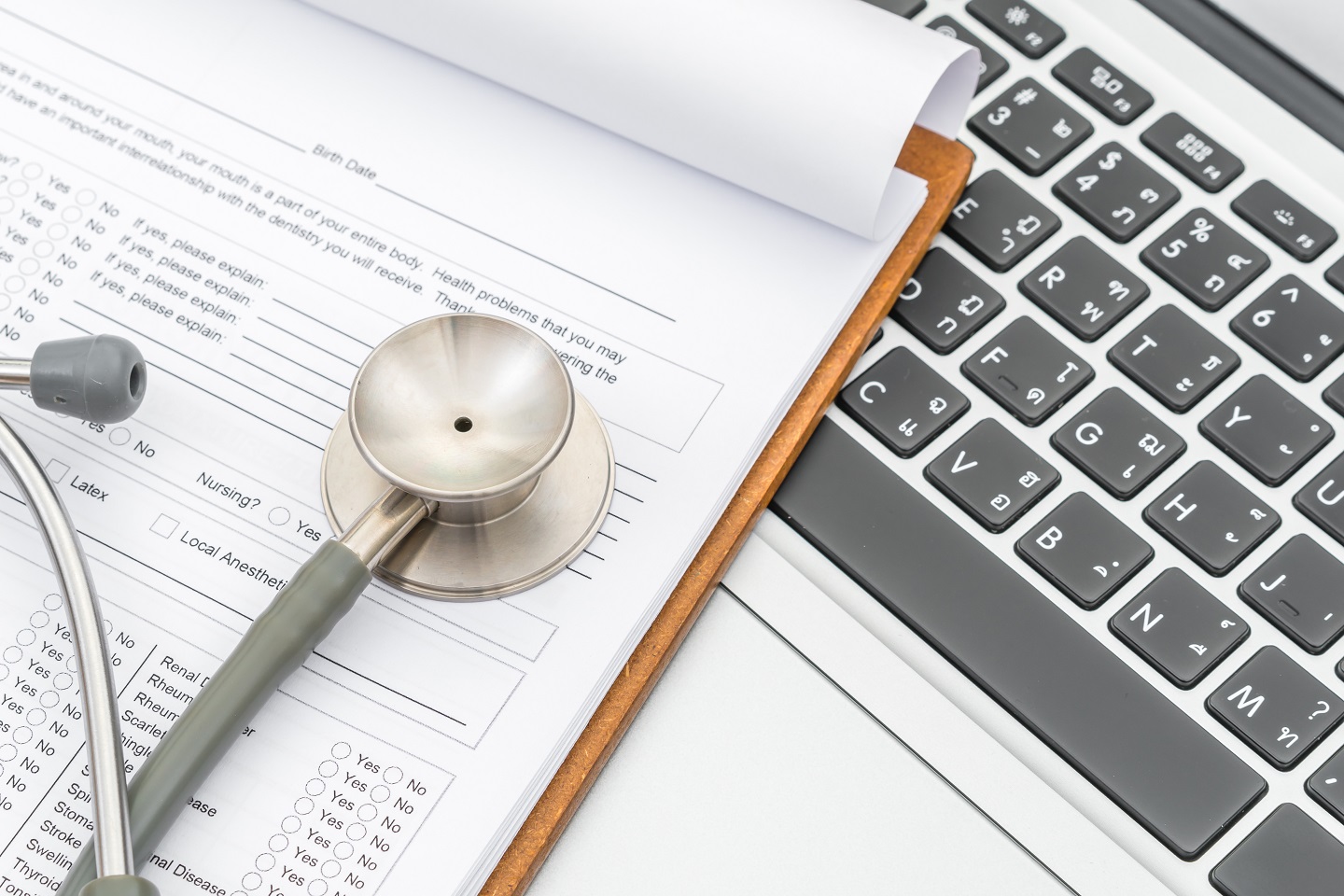
Screen new patients and check their eligibility by enabling online forms, and assign patients to specific trials based on predefined criteria.

Manage a patient database through a single gateway with controlled access, ensuring data security and easy retrieval of patient information.

Schedule appointments for research and clinical trials automatically, thanks to the integration with communication tools that message patients based on predefined triggers.

Track and maintain cases along the recruitment pipeline by sending follow-ups and notifications, ensuring continuous engagement with potential trial participants.
Get advanced reporting and analytics with various KPIs, such as the number of screened participants, patient conversion rate, and much more.

Integrate your patient recruitment software with EHR, patient engagement software, and other tools for a seamless and efficient workflow.

Belitsoft guarantees you have accurate, up-to-date information at your fingertips. Our cloud-based inventory management systems help you handle supplies more efficiently and meet your customers' needs. For legacy systems upgrades we integrate real-time ERP updates, barcode scanning, and e-commerce capabilities.

We design custom medical billing software for various healthcare organizations and provide all the necessary tools for efficient revenue cycle management from a single place. Our software enables seamless integration of EHR for automated billing — fast, easy, and on time.
Our team develops secure and compliant insurance claims management systems tailored to your needs. We convert legacy systems to modern platforms, refine existing front-ends and simplify processes to improve productivity. Your solutions are delivered high-quality, on time and within budget.


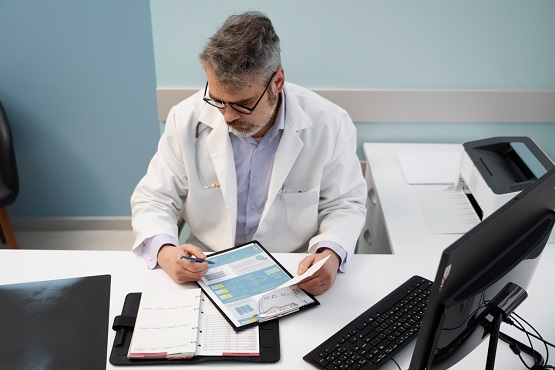
We create healthcare analytics databases and help manage and turn complex data in various healthcare fields into valuable insights. What is more, we expertly extract, clean, and transform the data to guarantee the utmost precision. Traditional EHR software can seamlessly integrate with our solutions.

We offer full support for developing visually appealing web portals in medical education that allow specialists to customize their online and offline learning and certification. Specialists can access educational resources, study remotely, attend live events, and receive certificates to demonstrate their knowledge.
HIPAA-Compliance
Database Interoperability
Relational Database
NoSQL Database
Custom EHR Databases
EHR Data Interoperability
EHR Security
300+ completed projects for various industries



Features for Healthcare Solutions
Speech Recognition
Artificial Intelligence & Machine Learning
Virtual & Augmented Reality
Gamification
Security
Other features
Mobile Apps for Healthcare Professionals
Belitsoft creates medical software applications, both for doctors and patients, and transfers the existing experience to a mobile environment. Our team is experienced in native iOS and Android development, as well as creating web and cross-platform mHealth solutions.
Mobile Apps for Healthcare Professionals
Mobile Apps for Patients
Why Belitsoft
We start the collaboration with the requirements analysis and the initial design discussions. Your app will look properly for both patients and doctors.
We believe you invest in building an extendable foundation platform. While developing the platform from scratch, we use custom technologies to ensure the right level of flexibility in the future.
We keep you informed and engaged with no burden on you. You get a comfortable project documentation process and the amount of calls per week.
We have a positive experience working with a focus group of active users throughout the health software development process. For example, our team allied with hospital workers to improve a software prototype and find new and, above all, necessary features to include in the MVP release.
At the outset of the project, we coordinate with a client on software compliance with health IT standards. Our teams work with different data exchange standards, such as HL7 and FHIR; DICOM and PACS for medical images; C-CDA for clinical document architecture and many others.
Belitsoft enters an NDA before we know the client’s project ideas. Experienced in working with security audit companies, we can confirm that the client’s medical software solution meets HIPAA and GDPR requirements.
Technologies and tools we use
Frequently Asked Questions
- building EHR and EMR systems
- patient portals
- medical practice management solutions
- inventory management systems
- ongoing medical education platforms
- and more
Recommended posts
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
Our Clients' Feedback













Belitsoft has been the driving force behind several of our software development projects within the last few years. This company demonstrates high professionalism in their work approach. They have continuously proved to be ready to go the extra mile. We are very happy with Belitsoft, and in a position to strongly recommend them for software development and support as a most reliable and fully transparent partner focused on long term business relationships.

Global Head of Commercial Development L&D at Technicolor
They use their knowledge and skills to program the product, and then completed a series of quality assurance tests. We were working in an agile way with them. Belitsoft performed very well throughout our project. We are definitely looking at Belitsoft as a long-term partner.

Service Delivery Director at Crimson (United Kingdom)
I highly recommend Belitsoft for website design and development. We were up against a tight deadline to launch the project. The work was delivered on time and within budget! I will continue working with Belitsoft as a valued partner for our web development!

Program Administrator at UC Berkeley (United States)
We have worked with Belitsoft team over the past few years on projects involving much customized programming work. They are knowledgeable and are able to complete tasks on schedule, meeting our technical requirements. We would recommend them to anyone who is in need of custom programming work.

Main Partner at Hathway Tech (United States)
Belitsoft company is able to make changes instantly. One of our internal engineers has commented about how clean their code is. Belitsoft seems to know what they're doing, which I appreciate.

Co-Founder at HOWCAST MEDIA (United States)
It was a great pleasure working with Belitsoft software development company. New requirements and adjustments were implemented fast and precisely. We can recommend Belitsoft and are looking forward to start a follow-up project.

Head of Division at Fraunhofer FIT (Germany)
Belitsoft company has been able to provide senior developers with the skills to support back end, native mobile and web applications. We continue today to augment our existing staff with great developers from Belitsoft.

CEO at Apollo Matrix (United States)
Belitsoft company delivered dedicated development team for our products, and technical specialists for our clients' custom development needs. We highly recommend to use this company if you want the same benefits.

Managing Director at Key2Know A/S in 2012 (Denmark)
We approached BelITsoft with a concept, and they were able to convert it into a multi-platform software solution. Their team members are skilled, agile and attached to their work, all of which paid dividends as our software grew in complexity.

COO at Regenerative Medicine LLC (United States)
Having worked with Belitsoft as a service provider, I must say that I'm very pleased with the company's policy. Belitsoft guarantees first-class service through efficient management, great expertise, and a systematic approach to business. I would strongly recommend Belitsoft's services to anyone wanting to get the right IT products in the right place at the right time.

CEO at Moblers
If you are looking for a true partnership Belitsoft company might be the best choice for you. They have proven to be most reliable, polite and professional. The team managed to adapt to changing requirements and to provide me with best solutions. I strongly recommend Belisoft.

Director at ShowCast Limited (Germany)
I expected and demanded a lot of you at Belitsoft company, but you exceeded my expectations. You acted pro-actively, challenged me at the right moments. Thanks!"

CEO at Ticken B.V. (Netherlands)
We have been working for over 10 years and they have become our long-term technology partner. Any software development, programming, or design needs we have had, Belitsoft company has always been able to handle this for us.
Founder from ZensAI (Microsoft)/ formerly Elearningforce